

")



Diagnostic capabilities of cardiac computed tomography in the preoperative diagnosis of hypertrophic cardiomyopathy
- Authors: Dariy O.Y.1,2, Yurpolskaya L.A.1, Rychina I.E.1, Dorofeev A.V.1, Golukhova E.Z.1
-
Affiliations:
- Bakulev Scientific Center for Cardiovascular Surgery
- Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
- Issue: Vol 5, No 3 (2024)
- Pages: 467-479
- Section: Original Study Articles
- URL: https://ogarev-online.ru/DD/article/view/310030
- DOI: https://doi.org/10.17816/DD629141
- ID: 310030
Cite item
Full Text

Abstract
BACKGROUND: A comprehensive approach to studying hypertrophic cardiomyopathy with diagnostic equipment and the latest scanning methods will ensure quality control and effective treatment of patients with this condition. The implementation of innovative technologies and computer calculation using next-generation scanners may become relevant and promising in studying various phenotypes of left ventricular remodeling in combination with abnormalities of the chordopapillary apparatus of the mitral valve and myocardial structure.
AIM: To examine the diagnostic capabilities of computed tomography in the preoperative examination of various hypertrophic cardiomyopathy phenotypes.
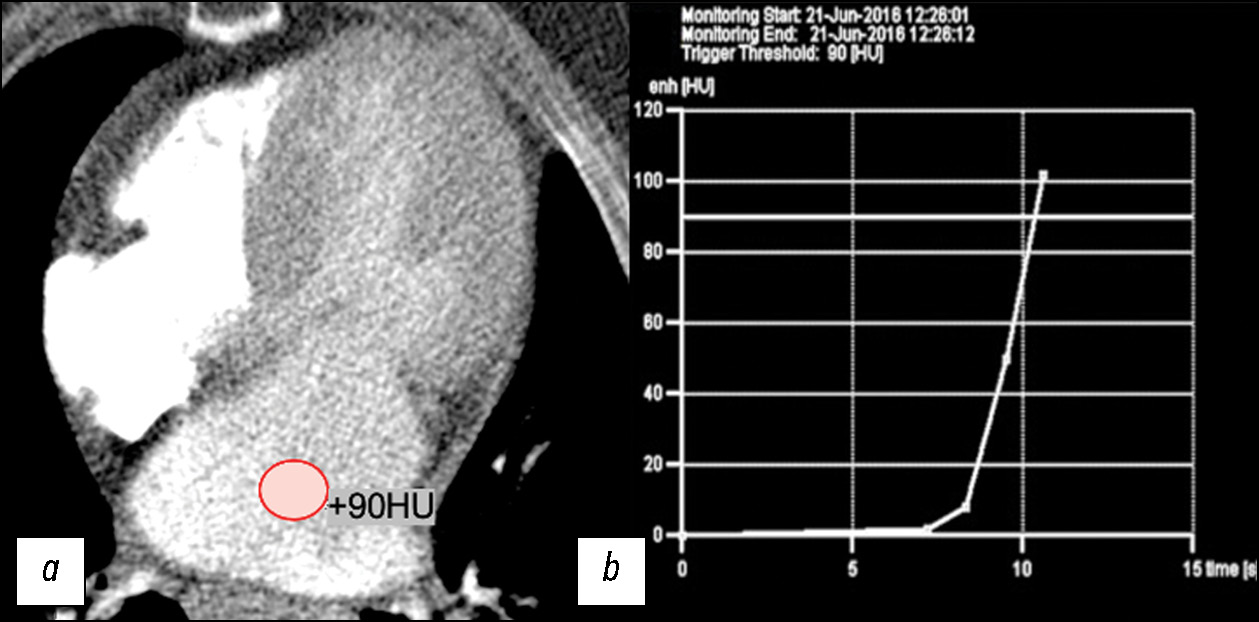
MATERIALS AND METHODS: The retrospective data analysis included 47 patients with hypertrophic cardiomyopathy (mean age, 52±7 full years) before surgical correction. computed tomography was performed using our protocol with automatic bolus tracking in the left atrium with a 90 HU threshold and biphasic contrast injection to assess the heart chambers and coronary arteries anatomy and mitral valve morphology. Moreover, to assess myocardial structure remodeling, iodine dual-energy computed tomography maps obtained with delayed contrast enhancement were analyzed. All patients with hypertrophic cardiomyopathy were classified by morphological types. The anatomy of chordopapillary apparatus was evaluated in each case.
RESULTS: This study demonstrated variability in hypertrophic cardiomyopathy phenotypes, which were conventionally divided into five morphological categories, but not restricted by them. Among the patients, 26 (55%) had diffuse septum hypertrophic cardiomyopathy, 5 (11%) had midventricular hypertrophic cardiomyopathy, 2 (4%) had midventricular obstruction and apical aneurysm, 8 (18%) had focal basal septum hypertrophic cardiomyopathy, 4 (8%) had concentric hypertrophic cardiomyopathy, and the remaining 4 (8%) had apical hypertrophic cardiomyopathy. Most patients were diagnosed with chordopapillary abnormalities of the mitral valve, categorized by papillary muscle number and position, and the ratio of chords to muscles. In 10 (21%) patients, data on the myocardial bridge of a coronary artery were obtained, whereas 3 (14%) of them had dynamic stenosis. All patients had focal iodine uptake on dual-energy computed tomography maps. An extracellular volume increase was observed in 10 out of 13 (76%) patients. As shown by dual-energy computed tomography, the mean extracellular volume of the left ventricular myocardium was 30.58% (95% confidence interval, 27–34%).
CONCLUSION: Our scanning protocols developed with computed tomography scanners of various generations enable to evaluate the specific morphological patterns of hypertrophic cardiomyopathy in a single study and provide a detailed interpretation of the geometry of cardiac valves and chambers, left ventricular function, state of the coronary bed, and structural changes of the left ventricular myocardium.
Full Text
##article.viewOnOriginalSite##About the authors
Olga Y. Dariy
Bakulev Scientific Center for Cardiovascular Surgery; Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Email: dariiolyka@mail.ru
ORCID iD: 0000-0003-0140-8166
SPIN-code: 1844-4944
MD, Cand. Sci. (Medicine)
Russian Federation, Moscow; MoscowLiudmila A. Yurpolskaya
Bakulev Scientific Center for Cardiovascular Surgery
Email: layurpolskaya@bakulev.ru
ORCID iD: 0000-0001-7780-2405
SPIN-code: 8436-9665
MD, Dr. Sci. (Medicine)
Russian Federation, MoscowInna E. Rychina
Bakulev Scientific Center for Cardiovascular Surgery
Email: ierychina@bakulev.ru
ORCID iD: 0000-0001-8056-4188
SPIN-code: 3516-0729
MD, Cand. Sci. (Medicine)
Russian Federation, MoscowAleksey V. Dorofeev
Bakulev Scientific Center for Cardiovascular Surgery
Email: avdorofeev@bakulev.ru
ORCID iD: 0000-0003-0833-9650
MD, Cand. Sci. (Medicine)
Russian Federation, MoscowElena Z. Golukhova
Bakulev Scientific Center for Cardiovascular Surgery
Author for correspondence.
Email: egolukhova@bakulev.ru
ORCID iD: 0000-0002-6252-0322
SPIN-code: 9334-5672
MD, Dr. Sci. (Medicine), Academician of Russian Academy of Science
Russian Federation, MoscowReferences
- Maron BJ, McKenna WJ, Danielson GK, et al. American College of Cardiology/European Society of Cardiology Clinical Expert Consensus Document on Hypertrophic Cardiomyopathy. J Am Coll Cardiol. 2003;42(9):1687–1713. doi: 10.1016/s0735-1097(03)00941-0
- Kotkar KD, Said SM, Dearani JA, Schaff HV. Hypertrophic obstructive cardiomyopathy: the Mayo Clinic experience. Ann Cardiothorac Surg. 2017;6(4):329–336. doi: 10.21037/acs.2017.07.03
- Ommen SR, Mital S, Burke MA, et al. 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients With Hypertrophic Cardiomyopathy: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circultation. 2020;142(25):e558–e631. doi: 10.1161/CIR.0000000000000937
- Brigden W. Uncommon myocardial diseases: the non-coronary cardiomyopathies. Lancet. 1957;273(7008):1243–1249. doi: 10.1016/s0140-6736(57)91537-4
- Choudhury L, Mahrholdt H, Wagner A, et al. Myocardial scarring in asymptomatic or mildly symptomatic patients with hypertrophic cardiomyopathy. J Am Coll Cardiol. 2002;40(12):2156–2164. doi: 10.1016/S0735-1097(02)02602-5
- Shiozaki AA, Senra T, Arteaga E, et al. Myocardial fibrosis detected by cardiac CT predicts ventricular fibrillation/ventricular tachycardia events in patients with hypertrophic cardiomyopathy. J Cardiovasc Comput Tomogr. 2013;7(3):173–181. doi: 10.1016/j.jcct.2013.04.002
- Qin L, Chen C, Gu S, et al. A radiomic approach to predict myocardial fibrosis on coronary CT angiography in hypertrophic cardiomyopathy. International Journal of Cardiology. 2021;337:113–118. doi: 10.1016/j.ijcard.2021.04.060
- Berliner JI, Kino A, Carr JC, Bonow RO, Choudhury L. Cardiac computed tomographic imaging to evaluate myocardial scarring/fibrosis in patients with hypertrophic cardiomyopathy: a comparison with cardiac magnetic resonance imaging. Int J Cardiovasc Imaging. 2013;29(1):191–197. doi: 10.1007/s10554-012-0048-y
- Bokeriya LA. Hypertrophic obstructive cardiomyopathy. Annals of Surgery (Russia). 2013;5:5–14. (In Russ).
- Baxi AJ, Restrepo CS, Vargas D, et al. Hypertrophic cardiomyopathy from A to Z: genetics, pathophysiology, imaging, and management. Radiographics. 2016;36:335–354. doi: 10.1148/rg.2016150137
- Efthimiadis GK, Pagourelias ED, Hadjimiltiades S, et al. Feasibility and significance of preclinical diagnosis in hypertrophic cardiomyopathy. Cardiol Rev. 2015;23(6):297–302. doi: 10.1097/CRD.0000000000000076
- Vasil’ev YuA, Semenov DS, Akhmad ES, et al. Peculiarities of magnetic resonance imaging in patients with implants and metal structures. Moscow: Obshchestvo s ogranichennoi otvetstvennost’yu «Izdatel’skie resheniya»; 2022. (In Russ.) EDN: WNQXXM
- Bandula S, White SK, Flett AS, et al. Measurement of myocardial extracellular volume fraction by using equilibrium contrast-enhanced CT: validation against histologic findings. Radiology. 2013;269(2):396–403. doi: 10.1148/radiology.13130130
- Bokeriya LA, Darii OYu, Makarenko VN, et al. Computed and magnetic resonance imaging of hypertrophic cardiomyopathy. Educational and methodological manual. Moscow: Natsional’nyi meditsinskii issledovatel’skii tsentr serdechno-sosudistoi khirurgii imeni A.N. Bakuleva; 2022. (In Russ.) EDN: MOGFHL
- Patel P, Dhillon A, Popovic Z, et al. Left ventricular outflow tract obstruction in hypertrophic cardiomyopathy patients without severe septal hypertrophy: implications of mitral valve and papillary muscle abnormalities assessed using cardiac magnetic resonance and echocardiography. Circ Cardiovasc Imaging. 2015;8(7):e003132. doi: 10.1161/CIRCIMAGING.115.003132
- Laaroussi L, Ben Halima A, Boukhris M. Left ventricular non-compaction associated with hypertrophic cardiomyopathy in the same patient. Kardiol Pol. 2017;75(4):397. doi: 10.5603/KP.2017.0064
- Wigle ED, Auger P, Marquis Y. Muscular subaortic stenosis: the initial left ventricular inflow tract pressure as evidence of outflow tract obstruction. Can Med Assoc J. 1966;95(16):793–797.
- Ramsheyi SA, Pargaonkar S, Lassau JP, Acar C. Morphologic classification of the mitral papillary muscles. J Heart Valve Dis. 1996;5(5):472–476.
- Kovalevskaya EA, Krylova NS, Poteshkina NG, et al. Clinical profile of patients with hypertrophic cardiomyopathy with myocardial ischemia in the absence of coronary atherosclerosis. The journal of general medicine. 2018;(4):36–42. EDN: VVQBKY
- Abadia A, Assen M, Martin S, et al. Myocardial extracellular volume fraction to differentiate healthy from cardiomyopathic myocardium using dual-source dual-energy CT. Journal of Cardiovascular Computed Tomography. 2020;14(2):162–167. doi: 10.1016/j.jcct.2019.09.008
- Vullaganti S, Levine J, Raiker N, et al. Fibrosis in Hypertrophic Cardiomyopathy Patients With and Without Sarcomere Gene Mutations. Heart Lung Circ. 2021;30(10):1496–1501. doi: 10.1016/j.hlc.2021.04.008
Supplementary files









