

")


自身免疫性垂体炎:COVID-19 大流行期间的病例观察
- 作者: Surovcev E.N.1,2, Zelter P.M.1,3, Kapishnikov A.V.1, Pyshkina Y.S.1
-
隶属关系:
- Samara State Medical University
- Diagnostic and treatment center of International institution for biological systems named after Sergey Berezin
- Meir Hospital
- 期: 卷 6, 编号 1 (2025)
- 页面: 178-186
- 栏目: 临床病例及临床病例的系列
- URL: https://ogarev-online.ru/DD/article/view/310066
- DOI: https://doi.org/10.17816/DD634533
- ID: 310066
如何引用文章

详细
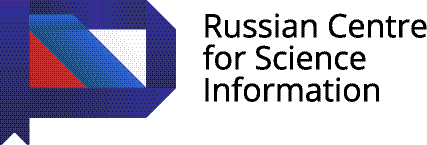
垂体炎是一种罕见的炎症性疾病,其特征是垂体及其柄的受累。该病可能由垂体组织浸润、自身免疫因素、感染性疾病或其他未明原因引起。由于某些垂体肿瘤(如垂体腺瘤和转移瘤)可能具有相似的临床特征,因此该病的临床诊断具有挑战性。磁共振成像是诊断疑似垂体炎以及鉴别腺垂体炎(前叶受累)与漏斗-神经垂体炎(垂体柄和后叶受累)的主要方法。垂体炎可分为原发性(自身免疫性)和继发性。继发性垂体炎可能继发于局灶性病变 (如肉芽肿、囊肿或腺瘤)或系统性疾病(如结节病、肉芽肿性多血管炎)。其临床表现受多种因素影响,其中之一是基础治疗。临床病例已有相关文献报道。
本文报道了一例 37 岁女性患者的临床病例,该患者既往诊断为高泌乳素血症,并接受卡麦角林对症治疗。患者被转诊进行磁共振成像检查,结果显示垂体信号不均匀。2021年7月随访磁共振成像显示垂体信号不均且增大。2021年12月,患者感染COVID-19并发生重度肺炎,接受糖皮质激素治疗及氧疗。2022年5月磁共振成像检查显示垂体明显增大且信号不均。在使用泼尼松(晨 10 mg,晚 5 mg)治疗后,患者的临床及影像学表现显著改善。
患者随访至COVID-19 大流行结束。对于此类患者,影像学结果的解读和治疗方案的选择可能受到新冠病毒感染及其治疗的影响。
在评估垂体炎的病程及其影像学变化时,医生应考虑 COVID-19 相关治疗,尤其是糖皮质激素对疾病的影响。
作者简介
Evgeniy N. Surovcev
Samara State Medical University; Diagnostic and treatment center of International institution for biological systems named after Sergey Berezin
Email: evgeniisurovcev@mail.ru
ORCID iD: 0000-0002-8236-833X
SPIN 代码: 5252-5661
MD, Cand. Sci. (Medicine)
俄罗斯联邦, Samara; TolyattiPavel M. Zelter
Samara State Medical University; Meir Hospital
Email: pzelter@mail.ru
ORCID iD: 0000-0003-1346-5942
SPIN 代码: 3678-3932
MD, Cand. Sci. (Medicine)
俄罗斯联邦, Samara; Kfar-Sava, IsraelAleksandr V. Kapishnikov
Samara State Medical University
Email: a.kapishnikov@gmail.com
ORCID iD: 0000-0002-6858-372X
SPIN 代码: 6213-7455
MD, Dr. Sci. (Medicine), Professor
俄罗斯联邦, SamaraYuliya S. Pyshkina
Samara State Medical University
编辑信件的主要联系方式.
Email: yu.pyshkina@yandex.ru
ORCID iD: 0000-0002-7241-6828
SPIN 代码: 4225-1020
MD, Cand. Sci. (Medicine), Assistant Professor
俄罗斯联邦, Samara参考
- Uccella S, Dottermusch M, Erickson L, et al. Inflammatory and infectious disorders in endocrine pathology. Endocr Pathol. 2023;34(4):406–436. doi: 10.1007/s12022-023-09771-3 EDN: XJTAXG
- Caturegli P. Autoimmune hypophysitis: an underestimated disease in search of its autoantigen(s). J Clin Endocrinol Metab. 2007;92(6):2038–2040. doi: 10.1210/jc.2007-0808
- Vorontsov AV, Babaeva DM, Vladimirova VP, et al. Clinical and radiological diagnosis of hypophysitis: a review of literature and own data. Problems of Endocrinology. 2022;68(2):16–33. doi: 10.14341/probl12777 EDN: LPMHZL
- Wright K, Kim H, Hill T, et al. Preoperative differentiation of hypophysitis and pituitary adenomas using a novel clinicoradiologic scoring system. Pituitary. 2022;25(4):602–614. doi: 10.1007/s11102-022-01232-0 EDN: XQPLFK
- Tsukamoto T, Miki Y. Imaging of pituitary tumors: an update with the 5th WHO classifications-part 2. Neoplasms other than PitNET and tumor-mimicking lesions. Jpn J Radiol. 2023;41(8):808–829. doi: 10.1007/s11604-023-01407-0 EDN: CGTFFL
- Tartaglione T, Chiloiro S, Laino ME, et al. Neuro-radiological features can predict hypopituitarism in primary autoimmune hypophysitis. Pituitary. 2018;21(4):414–424. doi: 10.1007/s11102-018-0892-4 EDN: GTNYNU
- Karrou M, Benyakhlef S, Alla A, et al. Clinical presentation and management of hypophysitis: an observational study of case series. Surg Neurol Int. 2021;12:304. doi: 10.25259/sni_454_2021 EDN: ZYMRCD
- Caturegli P, Lupi I, Landek-Salgado M, et al. Pituitary autoimmunity: 30 years later. Autoimmun Rev. 2008;7(8):631–637. doi: 10.1016/j.autrev.2008.04.016 EDN: MEPFHV
- Ravindran R, Carter JL, Kumar A, et al. Pre-test cortisol levels in predicting short synacthen test outcome: a retrospective analysis. Clin Med Insights Endocrinol Diabetes. 2022;15:11795514221093316. doi: 10.1177/11795514221093316 EDN: APQAJS
- Langlois F, Varlamov EV, Fleseriu M. Hypophysitis, the growing spectrum of a rare pituitary disease. J Clin Endocrinol Metab. 2022;107(1);10–28. doi: 10.1210/clinem/dgab672 EDN: YLEGQC
- Al Argan R, Ramadhan A, Agnihotram RV, et al. Baseline MRI findings as predictors of hypopituitarism in patients with non-functioning pituitary adenomas. Endocr Connect. 2021;10(11):1445–1454. doi: 10.1530/ec-21-0386 EDN: SQCXNL
补充文件







