

")


弥散加权全身成像与18F-前列腺特异性膜抗原-1007正电子发射计算机断层显像联合计算机断层扫描在前列腺癌骨转移检测中的诊断准确性比较评估
- 作者: Gelezhe P.B.1,2, Reshetnikov R.V.1, Blokhin I.A.1, Kodenko M.R.1
-
隶属关系:
- Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
- European Medical Center
- 期: 卷 6, 编号 2 (2025)
- 页面: 239-250
- 栏目: 原创性科研成果
- URL: https://ogarev-online.ru/DD/article/view/310213
- DOI: https://doi.org/10.17816/DD633391
- EDN: https://elibrary.ru/QXLAWR
- ID: 310213
如何引用文章
全文:

详细
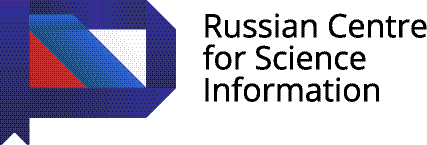
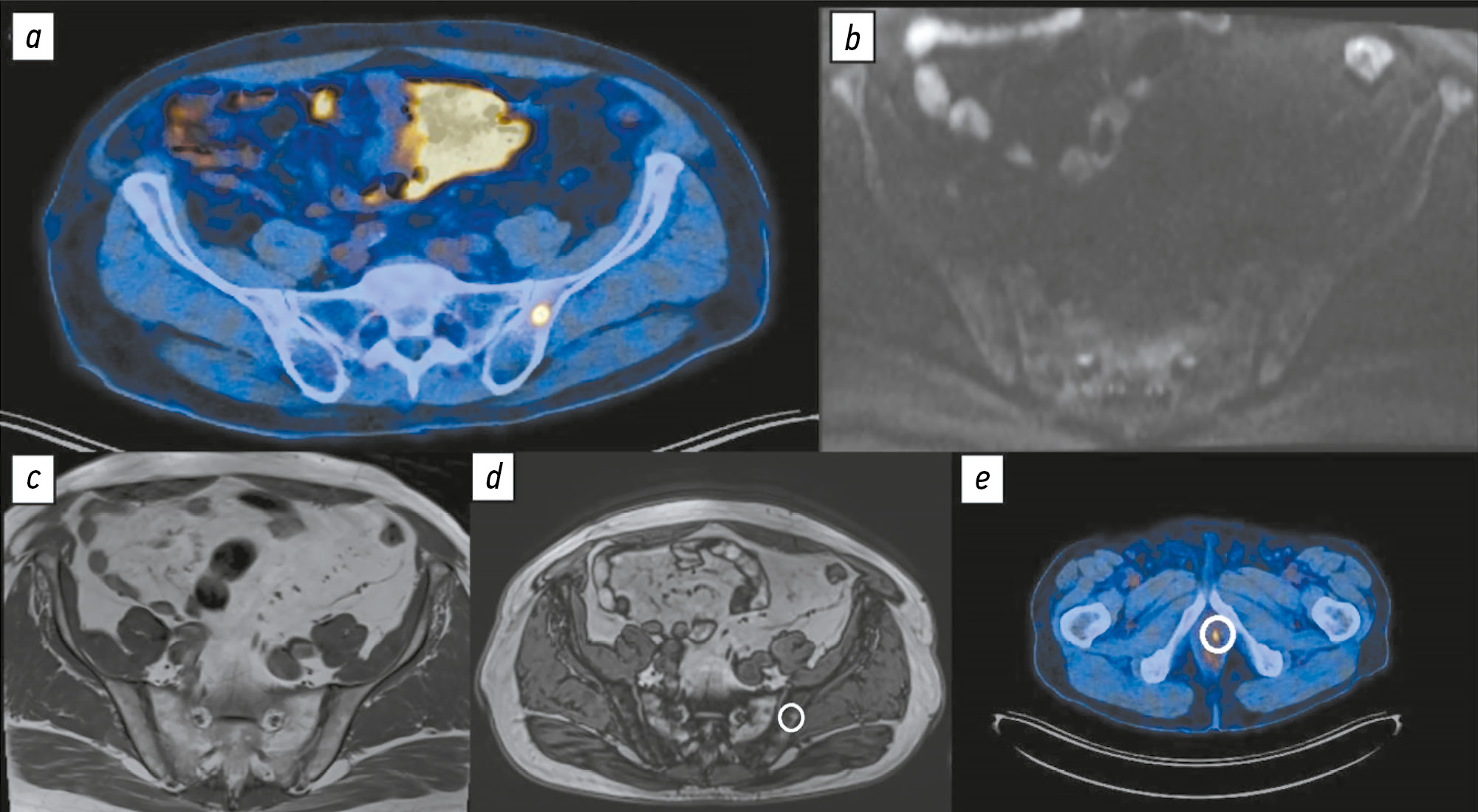
论证。随着18F-前列腺特异性膜抗原-1007(18F-PSMA-1007)在前列腺癌分期中的应用日益普及,其更高的空间分辨率逐渐显现出相对于其他同类示踪剂的优势。与此同时,越来越多研究指出,该示踪剂主要在骨组织中导致大量假阳性发现,从而可能引起肿瘤分期的不合理升高。弥散加权成像可作为骨转移早期诊断的一种方法。
目的:评估18F-PSMA-1007全身正电子发射计算机断层显像联合计算机断层扫描(PET/CT)在前列腺癌患者中,与全身及骨盆区域弥散加权成像相比,在骨转移检出方面的诊断准确性。
方法。本研究为一项回顾性、单中心抽样研究。共纳入119例前列腺癌患者的检查结果,并将其分为两组:第1组为40对18F-PSMA-1007 PET/CT与全身弥散加权成像磁共振检查数据;第2组为79对类似检查数据,其中磁共振检查仅限于骨盆区域。所有诊断性检查均在时间间隔不超过14天的前提下完成。根据18F-PSMA-1007 PET/CT和磁共振成像的结果,统计不同解剖部位检测到的骨转移灶数量。以磁共振成像的额外脉冲序列和/或动态随访结果作为依据,确认的病灶被视为真阳性。
结果。全身弥散加权成像在骨转移检出方面的特异性为58.1%,高于18F-PSMA-1007 PET/CT的51.06%。但敏感性略低,分别为93.22%和97.55%。
结论。尽管18F-PSMA-1007 PET/CT具有已知优势,但在骨骼中显示出较高的假阳性检出率。其最常见的累及部位为肋骨、椎骨和骨盆骨。为避免肿瘤分期被不当地提高,建议对可疑骨骼病灶进行进一步评估。可采用全身磁共振成像,结合弥散加权成像和选择性脂肪信号抑制序列,作为此类补充诊断方法。
关键词
作者简介
Pavel B. Gelezhe
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies; European Medical Center
编辑信件的主要联系方式.
Email: gelezhe.pavel@gmail.com
ORCID iD: 0000-0003-1072-2202
SPIN 代码: 4841-3234
MD, Cand. Sci. (Medicine)
俄罗斯联邦, Moscow; MoscowRoman V. Reshetnikov
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Email: ReshetnikovRV1@zdrav.mos.ru
ORCID iD: 0000-0002-9661-0254
SPIN 代码: 8592-0558
Cand. Sci. (Physics and Mathematics)
俄罗斯联邦, MoscowIvan A. Blokhin
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Email: BlokhinIA@zdrav.mos.ru
ORCID iD: 0000-0002-2681-9378
SPIN 代码: 3306-1387
俄罗斯联邦, Moscow
Maria R. Kodenko
Research and Practical Clinical Center for Diagnostics and Telemedicine Technologies
Email: KodenkoM@zdrav.mos.ru
ORCID iD: 0000-0002-0166-3768
SPIN 代码: 5789-0319
Cand. Sci. (Engineering)
俄罗斯联邦, Moscow参考
- Petersen LJ, Zacho HD. PSMA PET for primary lymph node staging of intermediate and high-risk prostate cancer: an expedited systematic review. Cancer Imaging. 2020;20(1):1–8. doi: 10.1186/s40644-020-0290-9 EDN: EWACNH
- Wondergem M, van der Zant FM, Broos WAM, Knol RJJ. Clinical impact of PSMA PET in biochemically recurrent prostate cancer; a review of the literature. Tijdschrift voor Urologie. 2020;10(6-7):109–121. doi: 10.1007/s13629-020-00296-6 EDN: XRLHSC
- Hofman MS, Lawrentschuk N, Francis RJ, et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): a prospective, randomised, multicentre study. The Lancet. 2020;395(10231):1208–1216. doi: 10.1016/s0140-6736(20)30314-7 EDN: IDQIFB
- Treglia G, Annunziata S, Pizzuto DA, et al. Detection rate of 18F-Labeled PSMA PET/CT in biochemical recurrent prostate cancer: a systematic review and a meta-analysis. Cancers. 2019;11(5):710. doi: 10.3390/cancers11050710
- Donswijk ML, van Leeuwen PJ, Vegt E, et al. Clinical impact of PSMA PET/CT in primary prostate cancer compared to conventional nodal and distant staging: a retrospective single center study. BMC Cancer. 2020;20(1):1–10. doi: 10.1186/s12885-020-07192-7 EDN: QXMNJG
- The FDA approves PSMAtargeted drug for PET imaging in men with prostate cancer. BJU International. 2021;127(3):267–268. doi: 10.1111/bju.15361
- Caribé PRRV, Koole M, D'Asseler Y, et al. NEMA NU 2-2007 performance characteristics of GE Signa integrated PET/MR for different PET isotopes. EJNMMI Physics. 2019;1(6):11. doi: 10.1186/s40658-019-0247-x
- Giesel FL, Hadaschik B, Cardinale J, et al. F-18 labelled PSMA-1007: biodistribution, radiation dosimetry and histopathological validation of tumor lesions in prostate cancer patients. European Journal of Nuclear Medicine and Molecular Imaging. 2016;44(4):678–688. doi: 10.1007/s00259-016-3573-4 EDN: RQYCMY
- Kroenke M, Mirzoyan L, Horn T, et al. Matched-pair comparison of 68Ga-PSMA-11 and 18F-rhPSMA-7 PET/CT in patients with primary and biochemical recurrence of prostate cancer: frequency of non–tumor-related uptake and tumor positivity. Journal of Nuclear Medicine. 2020;62(8):1082–1088. doi: 10.2967/jnumed.120.251447 EDN: EQTOAN
- Kwee TC, Takahara T, Ochiai R, et al. Diffusion-weighted whole-body imaging with background body signal suppression (DWIBS): features and potential applications in oncology. European Radiology. 2008;18(9):1937–1952. doi: 10.1007/s00330-008-0968-z EDN: BJSYMC
- Parker C, Tunariu N, Tovey H, et al. Radium-223 in metastatic castration-resistant prostate cancer: whole-body diffusion-weighted magnetic resonance imaging scanning to assess response. JNCI Cancer Spectrum. 2023;7(6):pkad077. doi: 10.1093/jncics/pkad077 EDN: AZWTFB
- Dresen RC, De Vuysere S, De Keyzer F, et al. Whole-body diffusion-weighted MRI for operability assessment in patients with colorectal cancer and peritoneal metastases. Cancer Imaging. 2019;19(1):1–10. doi: 10.1186/s40644-018-0187-z EDN: IEYSWA
- Yamamoto S, Yoshida S, Ishii C, et al. Metastatic diffusion volume based on apparent diffusion coefficient as a prognostic factor in castration-resistant prostate cancer. Journal of Magnetic Resonance Imaging. 2021;54(2):401–408. doi: 10.1002/jmri.27596 EDN: SFBRHR
- Rowe SP, Pienta KJ, Pomper MG, Gorin MA. PSMA-RADS Version 1.0: a step towards standardizing the interpretation and reporting of PSMA–targeted PET imaging studies. European Urology. 2018;73(4):485–487. doi: 10.1016/j.eururo.2017.10.027
- Vasilev YA, Omelyanskaya OV, Vladzymyrskyy AV, et al. Comparison of multiparametric and biparametric magnetic resonance imaging protocols for prostate cancer diagnosis by radiologists with different experience. Digital Diagnostics. 2023;4(4):455–466. doi: 10.17816/dd322816 EDN: PVEPWX
- Disler DG, McCauley TR, Ratner LM, et al. In-phase and out-of-phase MR imaging of bone marrow: prediction of neoplasia based on the detection of coexistent fat and water. American Journal of Roentgenology. 1997;169(5):1439–1447. doi: 10.2214/ajr.169.5.9353477
- Suh CH, Yun SJ, Jin W, et al. Diagnostic Performance of in-phase and opposed-phase chemical-shift imaging for differentiating benign and malignant vertebral marrow lesions: a meta-analysis. American Journal of Roentgenology. 2018;211(4):W188–W197. doi: 10.2214/AJR.17.19306
- Halpern SD. The continuing unethical conduct of underpowered clinical trials. JAMA. 2002;288(3):358–362. doi: 10.1001/jama.288.3.358
- Altman DG. Statistics and ethics in medical research: III How large a sample? BMJ. 1980;281(6251):1336–1338. doi: 10.1136/bmj.281.6251.1336
- Blokhin IA, Kodenko MR, Shumskaya YuF, et al. Hypothesis testing using R. Digital Diagnostics. 2023;4(2):238–247. doi: 10.17816/DD121368 EDN: OEKDAG
- Grünig H, Maurer A, Thali Y, et al. Focal unspecific bone uptake on [18F]-PSMA-1007 PET: a multicenter retrospective evaluation of the distribution, frequency, and quantitative parameters of a potential pitfall in prostate cancer imaging. European Journal of Nuclear Medicine and Molecular Imaging. 2021;48(13):4483–4494. doi: 10.1007/s00259-021-05424-x
- Silver DA, Pellicer I, Fair WR, et al. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin Cancer Res. 1997:3(1):81–85.
- Plouznikoff N, Garcia C, Artigas C, et al. Heterogeneity of 68Ga-PSMA PET/CT uptake in fibrous dysplasia. Clinical Nuclear Medicine. 2019;44(10):e593–e594. doi: 10.1097/RLU.0000000000002609
- Gossili F, Lyngby CG, Løgager V, Zacho HD. Intense PSMA uptake in a vertebral hemangioma mimicking a solitary bone metastasis in the primary staging of prostate cancer via 68Ga-PSMA PET/CT. Diagnostics. 2023;13(10):1730. doi: 10.3390/diagnostics13101730 EDN: HQPGMR
- Hoyle JM, Layfield LJ, Crim J. The lipid-poor hemangioma: an investigation into the behavior of the “atypical” hemangioma. Skeletal Radiology. 2020;49:93–100. doi: 10.1007/s00256-019-03257-2
- Liao Z, Liu G, Ming B, et al. Evaluating prostate cancer bone metastasis using accelerated whole-body isotropic 3D T1-weighted Dixon MRI with compressed SENSE: a feasibility study. European Radiology. 2023;33(3):1719–1728. doi: 10.1007/s00330-022-09181-9
- Park S, Park JG, Jun S, et al. Differentiation of bone metastases from prostate cancer and benign red marrow depositions of the pelvic bone with multiparametric MRI. Magnetic Resonance Imaging. 2020;73:118–124. doi: 10.1016/j.mri.2020.08.019 EDN: CTHKSL
- Lee JH, Park S. Differentiation of schmorl nodes from bone metastases of the spine: use of apparent diffusion coefficient derived from DWI and fat fraction derived from a Dixon sequence. American Journal of Roentgenology. 2019;213(5):W228–W235. doi: 10.2214/AJR.18.21003
- Hottat NA, Badr DA, Ben Ghanem M, et al. Assessment of whole-body MRI including diffusion-weighted sequences in the initial staging of breast cancer patients at high risk of metastases in comparison with PET-CT: a prospective cohort study. European Radiology. 2023;34(1):165–178. doi: 10.1007/s00330-023-10060-0 EDN: MRFKMJ
- Johnston EW, Latifoltojar A, Sidhu HS, et al. Multiparametric whole-body 3.0-T MRI in newly diagnosed intermediate- and high-risk prostate cancer: diagnostic accuracy and interobserver agreement for nodal and metastatic staging. European Radiology. 2018;29(6):3159–3169. doi: 10.1007/s00330-018-5813-4 EDN: DEXLFX
- Liu F, Dong J, Shen Y, et al. Comparison of PET/CT and MRI in the diagnosis of bone metastasis in prostate cancer patients: a network analysis of diagnostic studies. Frontiers in Oncology. 2021;11(APR):736654. doi: 10.3389/fonc.2021.736654 EDN: TKTQOV
- Nakanishi K, Tanaka J, Nakaya Y, et al. Whole-body MRI: detecting bone metastases from prostate cancer. Japanese Journal of Radiology. 2021;40(3):229–244. doi: 10.1007/s11604-021-01205-6 EDN: QZBDSB
- Sun W, Li M, Gu Y, et al. Diagnostic value of whole-body DWI with background body suppression plus calculation of apparent diffusion coefficient at 3 T Versus 18F-FDG PET/CT for detection of bone metastases. American Journal of Roentgenology. 2020;214(2):446–454. doi: 10.2214/ajr.19.21656 EDN: BJRCLP
- Larbi A, Omoumi P, Pasoglou V, et al. Whole-body MRI to assess bone involvement in prostate cancer and multiple myeloma: comparison of the diagnostic accuracies of the T1, short tau inversion recovery (STIR), and high b-values diffusion-weighted imaging (DWI) sequences. European Radiology. 2018;29(8):4503–4513. doi: 10.1007/s00330-018-5796-1 EDN: CEOKNS
- Chen B, Wei P, Macapinlac HA, Lu Y. Comparison of 18F-Fluciclovine PET/CT and 99mTc-MDP bone scan in detection of bone metastasis in prostate cancer. Nuclear Medicine Communications. 2019;40(9):940–946. doi: 10.1097/MNM.0000000000001051 EDN: ZRPGWP
- Gelezhe P.B. Comprehensive diagnostics of breast cancer using magnetic resonance imaging and positron emission tomography with 18F-fluorodeoxyglucose, combined with computed tomography [dissertation]. Moscow; 2020. Available from: https://www.elibrary.ru/item.asp?id=54413422 EDN: UGEBZO
- Freitag MT, Radtke JP, Hadaschik BA, et al. Comparison of hybrid 68Ga-PSMA PET/MRI and 68Ga-PSMA PET/CT in the evaluation of lymph node and bone metastases of prostate cancer. European Journal of Nuclear Medicine and Molecular Imaging. 2015;43(1):70–83. doi: 10.1007/s00259-015-3206-3 EDN: HXYHGT
补充文件



